JOHN A. KOLMER, M.D., LL.D.,Sc.D. Professor of Medicine, Temple University School of Medicine, and Director of the Research Institute of Cutaneous Medicine
WITH THE ASSISTANCE OF
GEORGE F. KLUGH JR., M.D. Resident in Medicine, Temple University Hospital
AND
MISS ANNA M. RULE, PHILADELPHIA
Journal of the American Medical Association 104 no. 6 (Feb. 9, 1935): 456-460
Owing to the fact that it appears that living vaccines of attenuated viruses are more vaccinogenic than heat or chemically killed viruses, we employed sodium ricinoleate (William Merrell Company) as the attenuating agent not only because it is known to be detoxifying, but likewise because McKinley and Larson had successfully immunized three monkeys completely and one partially with intraperitoneal injections of sodium ricinoleate treated emulsions of monkey spinal cord virus. At least it would appear that vaccines of attentuated viruses produce immunity in much smaller amounts than "dead" viruses, with the added advantage that the viruses after injection are probably able to multiply many fold with continued antigenic stimulation as well as requiring the injection of smaller amounts of spinal cord protein and thereby resulting in less strain on the antibody producing tissues and less likelihood of producing allergic sensitization.
Furthermore, marked success in the case of poliomyelitis has followed vaccination of monkeys with subcutaneous and intracutaneous injections of living virus or mixtures of virus and immune serum, but these have been considered too dangerous for the vaccination of human beings.
Susceptibility, attack rate, mortality and incidence of residual paralysis and other factors in acute poliomyelitis in relation to vaccination of human beings have been discussed elsewhere, it being pointed out that susceptibility is so high in children and especially among those under 10 years of age that a safe and effective method of vaccination is highly desirable and especially in epidemics, although the majority of adults appear to possess adequate resistance. Even among the latter, however, vaccination is worthy of serious consideration during epidemics at least, since serum neutralization tests by different investigators with a group of 128 varying in age from 15 years and upward has shown about 24.7 per cent without demonstrable amounts of neutralizing antibody in the blood.
METHOD OF STUDY
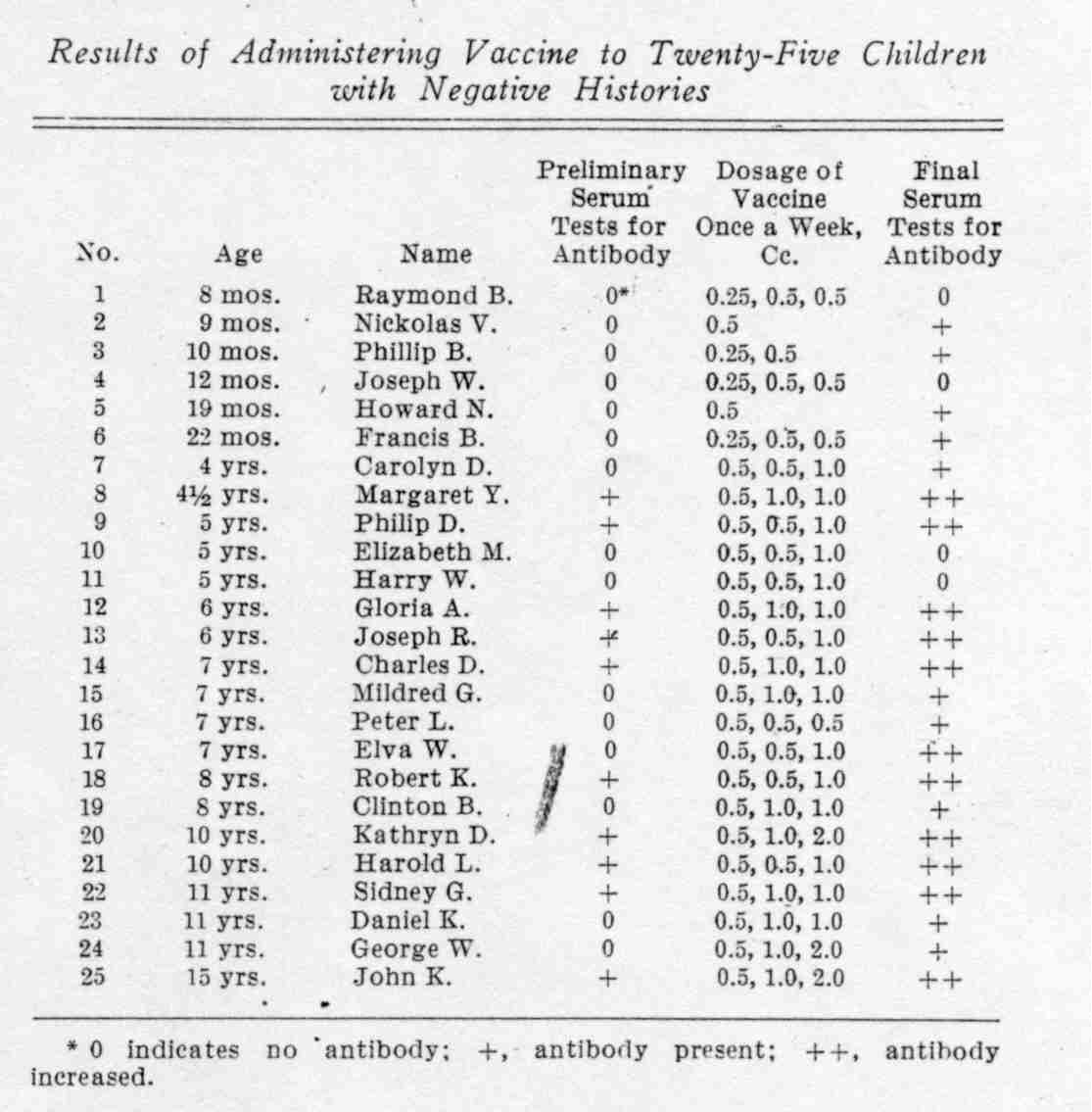
During the last four months we have administered the vaccine to a selected group of twenty-five children varying in age from 8 months to 15 years as summarized in the table, with completely negative histories of clinical attacks of poliomyelitis. All were immunized at the request or with the written consent of the parents, nineteen being in Temple University Hospital in the pediatric service of Dr. Ralph M. Tyson, to whom we are indebted for this cooperation. While all these children were in fairly good health, the majority were convalescing from various medical and surgical ailments.
Fifteen of these children were selected on the basis of showing no antibody in the blood by serum neutralization tests and ten with antibody in order to include both types in the study. These tests were conducted by mixing 0.5 cc. of serum with 0.5 cc. of a 10 per cent suspension of virus followed by intracerebral injection of 0.5 cc. of each mixture into monkeys under ether anesthesia after being allowed to stand about two hours in a water bath at 37 C. Control monkeys injected with 0.5 cc. of a mixture of 0.3 cc. of sterile saline solution and 0.5 cc. of virus after standing under identical conditions developed paralysis in from five to nine days.
Temperature observations and blood examinations were made in twenty-two of the children before and after each dose of vaccine.
From one to three injections were given subcutaneously at weekly intervals, the amounts of each being shown in the table.
RESULTS OF VACCINATION
There were no ill effects in any of the children, and not the slightest evidences of infection. Local reactions of varying degree occurred at the sites of infection. In one of the older children the first dose produced a moderately severe reaction of swelling and erythema corresponding to that sometimes seen following injections of diphtheria toxoid, but in the remainder the local reactions were of mild degree.
During the first twenty-four hours after injection and especially after the first, the temperature of some of the children was elevated to a fraction of a degree but only occasionally going as high as 100.2 F. and falling to the preinjection levels in about forty-eight hours.
The total leukocytes were increased from 500 to 1,200 per cubic millimeter of blood in some of the children during twenty-four hours following injections and especially after the first, as the result of a slight absolute increase of the polymorphonuclear neutrophils. These and the slight temperature changes were ascribed to the effects of the local reactions, as they appeared to vary with the degree of the latter.
Serum neutralization tests for antibody were conducted one week after the last dose of vaccine by mixing 0.5 cc. of serum with 0.5 cc. of a 10 per cent suspension of virus, allowing it to stand at 37 C. for but one to two hours, and injecting 0.5 cc. of each mixture intracerebrally into monkeys under ether anesthesia.
In the fifteen children without antibody before immunization, eleven, or 75 per cent, showed sufficient amounts of antibody to neutralize the virus after immunization, the monkeys showing absolutely no evidences of infection over three to four weeks following intracerebral inoculation of the serum-virus mixtures, while the controls inoculated with but 0.1 cc. of virus alone became paralyzed in from six to nine days and succumbed.
Since Brodie has recently shown that the maximum immunity from two intracutaneous doses of poliomyelitis virus in monkeys is obtained by giving the second while the first is giving its effects, in other words, at intervals of from ten to fourteen days apart, it is quite likely that our injections at weekly intervals were too closely spaced and that even better results might have been produced by giving the injections at longer intervals. Furthermore, while antibody production in some of the children appeared to be quite prompt after injections of the vaccine, as will be dis- cussed shortly in more detail, it is likely that serum neutralization tests for antibody should be delayed for at least two weeks after the last dose instead of but one week as conducted by us.
In addition it should be stated as previously mentioned that the majority of children included in this group were convalescing in the hospital from various medical and surgical conditions with the possibility that antibody response may not be as good under the circumstances, as occurs in children in excellent general health.
Despite these conditions, however, the production of large amounts of antibody in eleven out of fifteen, or 75 per cent, of susceptible antibody-free children by from one.to three doses of vaccine, with absolutely no ill effects other than the slight local reactions at the sites of subcutaneous injection, indicates a satisfactory and successful degree, of immunization.
Furthermore, the serums of the ten children containing antiviral antibody in the blood before vaccination showed a sharp increase of antibody after immunization, since 0.5 cc. of serum mixed with as much as 0.5 cc. of 50 per cent-suspension of virus followed by the intracerebral injection into monkeys under eiher anesthesia of 0.5 cc. of the mixtures, after standing but one to two hours at 37 C., showed complete neutralization. Indeed, it would appear from additional quantitative tests that the vaccine probably produces more antibody in those children carrying natural antibody in the blood than it does in those who do not, suggesting that the body cells in the former are probably sensitized or "tuned up" by previous unrecognized infection with virus, with the result that they produce large additional amounts of antibody on additional stimulation by vaccine. At least twenty-one, or 84 per cent of the group of twenty-five children, showed good antibody response to the vaccine.
DOSAGE OF VACCINE
The matter of dosage is of course one of considerable importance. Monkeys receiving a total of 0.5 cc. per kilogram in divided doses by subcutaneous injection have been successfully vaccinated; but, if it is true that human beings acquire immunity to poliomyelitis by clinically unrecognized infection with virus, it would appear that less vaccine may be required per body weight for effective immunization than in the case of monkeys.
With this possibility in mind and as an additional factor of safety, we have made the first dose 0.25 cc. for children under 3 years of age and 0.5 cc. for older children and adults. Second doses have varied from 0.5 to I cc. and third doses 1 or 2 cc., as shown in the table.
From the results observed up to the present time, it would appear that three doses are sufficient in the following amounts:
- From 1 to 3 years: first, 0.25 cc.; second, 0.5 cc.; third, 0.5 cc.
- From 4 to 10 years: first, 0.5 cc.; second, 0.5 cc.; third, 1cc.
- From 11 to 15 years: first, 0.5 cc.; second, 1cc.; third, 1 or 2 cc
- Adults: first, 0.5 cc.; second, 1cc.; third, 2 cc.
For children of standard weight the totals of these amounts of vaccine varied from about 0.06 to 0.1 cc. per kilogram which were therefore approximately five to ten times less per body weight than given to monkeys. But we have assumed, as stated before, that human beings may require less than monkeys per kilogram of weight, and the results summarized in the table appear to substantiate this assumption. A possible exception was in the case of the two children (1 and 4) of 8 and 12 months respectively, who probably should have received 1 cc. for the third dose instead of 0.5 cc.; but otherwise we believe that the foregoing scale is about right in view of our present information on this subject.
However, it would appear that but one or two doses of vaccine have produced considerable antibody in at least some of the children.
For example, the serums of Nickolas V. (patient 2), aged 9 months, and Howard N. (patient 5), aged 19 months, gave good neutralization tests four days after one dose of 0.5 cc. Joseph W. (patient 4), aged 12 months, gave a good neutralization test one week after the second dose, although this result was not known when the third dose was given, and Clinton B. (patient 19), aged 8 years, also gave a good neutralization test four days after the first dose of 0.5 cc., although the second and third doses were also given before this result was known. These results indicate that with some children at least one or two doses may suffice; but since Raymond B. (patient 1), Phillip B. (patient 3) and Francis B. (patient 6) did not show antibody in the serums one week after the first dose, we believe it is advisable to give two and preferably three doses of the vaccine.
RAPIDITY OF ANTIBODY PRODUCTION AND SPACING OF INJECTIONS
In view, however, of Dr. Brodie's observations previously referred to on the rate of production of antibody in monkeys given subinfective doses of living virus intracutaneously, it would appear advisable to give the injections every ten days instead of every seven days as we gave them.
On the other hand, we have observed rather rapid antibody production in the cases just referred to, namely, Nickolas V. (patient 2), Howard N. (patient 5) and Clinton B. (patient 19), since their serums taken ninety-six hours after the first dose of vaccine gave good neutralization tests. Indeed, in the case of Nikolas V., serum taken forty-eight hours after the first dose of vaccine appeared to contain already a very slight amount of antibody, as this monkey did not develop paralysis until eighteen days after intracerebral inoculation, whereas the control monkey and that tested with serum before vaccine was given developed severe paralysis thirteen or fourteen days after inoculation.
Further evidence of rather rapid antibody production was indicated by the fact that a monkey weighing 4 kg. infected intracerebrallv under ether anesthesia with 0.5 cc. of 5 per cent virus seventy-two hours after a subcutaneous injection of 0.5 cc. of vaccine remained perfectly well and entirely free of infection, whereas a control developed paralysis eight days after inoculation with but 0.1 cc. of the same virus given at the same time. In the case of a second monkey, however, receiving the same dose of vaccine, the antibody response, while present, was not quite as good, as this animal developed paralysis about nineteen days after the intracerebral injection under ether anesthesia of 0.5 cc. of the 5 per cent virus.
In this connection, observations on the rapidity of antibody production with the serums of individuals and monkeys with poliomyelitis are not without interest and some bearing on this question. Flexner and Amoss, for example, have found antibody in the serum as early as the sixth day of the disease; Amoss has found it in monkeys as early as three and one-half days after the onset of paralysis and in human beings as early as the fifth day; Leiner and von Wiesner found it after seven, and in one case two days after the development of active disease in monkeys. Brodie also found antibody in the blood of monkeys on the second day after the height of paralysis, while Howitt failed to find it earlier than fifteen days after the onset of the disease in monkeys.
On the whole, therefore, it would appear that antibody may be produced rather rapidly in poliomyelitis and after subcutaneous injections of the vaccine, and for this reason we believe that vaccination may prove particularly helpful in the immunization of individuals during epidemics. Furthermore, as has been discussed elsewhere, it does not appear that the vaccine produces a detectable "negative phase" or period of increased susceptibility in monkeys. at least, which also appears to ustify its use in combating epidemics of poliomyelitis.
THE VACCINE
The method of preparing the vaccine has already been described and need not be here given. Suffice it to emphasize that it is prepared of a remote monkey passage strain of the virus with the possibility of having lost at least some of its infectivity for human beings. That the antibody it produces is capable of neutralizing human virus is indicated by the fact that the antibody in the serums of several of the vaccinated children was found to neutralize completely human virus from the 1934 epidemic in California sent us by Dr. Jessel of Los Angeles and a second virus in the third monkey transfer sent by Miss Howitt of San Francisco.
The vaccine, however, cannot be prepared of brain tissue because it contains insufficient virus. The intracerebral inoculation of monkeys with as much as I cc. of a 50 per cent suspension of fresh brain has failed to infect because virus was absent or present in insufficient amounts. But the spinal cord of one monkey will furnish about 150 cc. of vaccine, which is sufficient for the immunization of from forty to seventy-five children, depending on age and dosage.
We believe that the virus in the vaccine is attenuated to some extent by the amounts of sodium ricinoleate employed. While the intracerebral injection into monkeys under ether anesthesia of 0.1 cc. of 5 per cent fresh virus produced poliomyelitis in about eight days, the intracerebral injection of 0.2 cc. of a vaccine 3 weeks old and carrying 4 per cent of virus produced poliomyelitis in eleven days, while a second vaccine 2 months old produced paralysis in nine days and a third about 5 months old in about twelve days, all being injected in doses of 0.2 cc. under ether anesthesia.
The vaccine is allowed to stand at least two weeks before use and we now believe that a month may be better. After this time attentuation of the vaccine appears to stop when kept in the refrigerator at about 10 C., since vaccine prepared a year ago still possesses about the same infectivity for the monkey and the same vaccinogenic activity. In order to render different vaccines comparable in attenuated virus and immunizing activity, they are now prepared of mixtures of from ten to twenty cords taken only from monkeys that have been severely paralyzed.
In the preparation of the vaccine, due care must be exercised against contamination of the cords in removal and the preparation of finely divided suspensions. But it is our custom to place the cords in 50 per cent chemically pure glycerol in sterile saline solution for at least a month before use and under the circumstances the great majority of vaccines are found to be sterile on careful bacteriologic examination by culture.
The 1 per cent sodium ricinoleate possesses some bacteriostatic activity, but due care must be exercised against contamination of the vaccine when administered.
Since we have never seen the slightest ill effects, aside from mild local reactions at the sites of injection in monkeys or the twenty-seven human beings including two of us (J. A. K. and A. M. R.) who have taken it, we lost all fear of infection from its administration and are sure that it is perfectly safe. Unfortunately the monkey serum neutralization test is the only one available at present for the detection of susceptibility, since skin tests, colloidal gold, complement fixation and precipitation tests have proved inadequate; but the majority of children under 10 years of age are devoid of antiviral antibody and probably susceptible, and since Aycock has shown that there is an important hereditary factor in susceptibility it would appear particularly important to vaccinate all children in those families in which the disease has appeared.
Not only is it quite likely that the remote passage virus employed has
lost some if not all infectivity for human beings, but it is certainly
attenuated to some extent by the sodium ricinoleate employed. Furthermore,
subcutaneous injections appear to add another very important factor of
added safety, as it represents a portal of entry in which virulent virus
itself has a very low rate of infectivity for monkeys. In addition
the injection of such a small first dose as from 0.25 to 0.5 cc to children
and adults and waiting at least a week before the second dose is given
adds another important factor of safety, since it appears that antibody
response is quite prompt. For these reasons we do not hesitate recommending
the vaccine, especially during epidemics, and among the first children
to receive it were the two sons of the senior author, the
younger of whom was without any antibody at all in his serum before the
first dose of 0.5 cc. was given.
SUMMARY
1. Twenty-five children varying in age from 8 months to 15 years have
been given from one to three injections of poliomyelitis vaccine at the
request or with the consent of parents.
2. Fifteen of these children were without antibody in serum neutralization
tests before immunization and eleven, or 75 per cent, showed large amounts
of antibody in the blood one week after the last dose of vaccine.
3. Ten of the children showed the presence of antiviral antibody in the
blood before immunization, but all have shown a considerable increase
of this antibody after vaccination, so that antibody production occurred
in twenty-one, or 84 per cent, of the group of twenty-five children.
4. None of the twenty-five children have shown the slightest ill effects
from the vaccine.
5. Mild local reactions were produced at the sites of subcutaneous injection,
with occasional slight elevation of temperature and slight leukocytosis
subsiding within forty-eight hours.
6. The dosage for children from 1 to 3. years of age has been 0.25, 0.5
and 0.5 cc. at weekly intervals; for children from 4 to 1 0 years, 0.
5, 0.5 and 1 cc.; f or children from 11 to 15 years, 0.5, 1 and 1 or 2
cc. For adults the dosage recommended is 0.5, 1 and 2 cc.
7. The vaccine is prepared-of spinal cord only, as
brain contains too small amounts of virus. But the spinal cord of a single
monkey will furnish about 150 cc. of vaccine, which is sufficient for
the immunization of from forty to seventy-five children, depending on
age and dosage
8. It is likely that the maximum antibody response may be obtained by
giving the injection every ten days instead of weekly.
9. Antibody production, however, appears to be fairly rapid, as three
susceptible children developed antibody in the blood within four days
after the first injection of vaccine and one monkey was found completely
and a second partially immune seventy-two hours after the subcutaneous
injection of 0.5 cc. of vaccine per animal on intracerebral inoculations
of large amounts of virus.
10. The vaccine does not appear to produce a demonstrable "negative
phase" of increased susceptibility after injection.
11. The vaccine is a 4 per cent suspension of spinal
cords of monkeys developing poliomyelitis after intracerebral inoculation
with a remote passage strain of virus, in a 1 per cent sterile solution
of sodium ricinoleate prepared as previously described. The virus is attenuated
and the vaccine regarded as entirely safe for the immunization of human
beings not only because prepared of remote passage virus which probably
has lost infectivity for human beings but likewise because of attenuation
by sodium ricinoleate, the route of administration and the injection of
a small first dose.
12. The amound of antibody produced by immunizations is comparable
to that found in the blood in natural immunity and is believed to be sufficient
for affording protection against acute anterior poliomyelitis.
13. The antibody present in the serums of vaccinated children has successfully
neutralized human virus from the 1934 California epidemic.
14. The duration of the immunity following vaccination is unknown but
has lasted for more than two years in vaccinated monkeys.
15. It is believed that the vaccine is now ready for vaccination of human
beings and especially children against poliomyelitis and particularly
during epidemics.
Copyright © 1997 University
of Pennsylvania HSS
Revised: